
Revisión sistemática de instrumentos
que evalúan la calidad de aplicaciones móviles de salud
Systematic review of instruments that assess the quality of
mobile health applications

 Claudio
Delgado-Morales. Personal investigador en
formación. Universidad de Huelva, España
Claudio
Delgado-Morales. Personal investigador en
formación. Universidad de Huelva, España
 Dra. Ana
Duarte-Hueros. Profesora Titular de Universidad.
Universidad de Huelva, España
Dra. Ana
Duarte-Hueros. Profesora Titular de Universidad.
Universidad de Huelva, España
Recibido:
2023/01/12 Revisado:2023/01/28 Aceptado: 2023/03/30 Preprint: 2023/04/13 Publicado:2023/05/01
Cómo citar este artículo:
Delgado-Morales,
C., & Duarte-Hueros, A. (2023). Revisión sistemática de instrumentos que
evalúan la calidad de aplicaciones móviles de salud [Systematic review of
instruments that assess the quality of mobile health applications]. Pixel-Bit.
Revista de Medios y Educación, 67, 35-58. https://doi.org/10.12795/pixelbit.97867
RESUMEN
En los últimos años ha aumentado
significativamente la descarga de aplicaciones móviles (apps) orientadas a
desarrollar hábitos saludables en la población en general. No obstante, la
mayoría no están sujetas a procesos de regulación de calidad, y los
instrumentos de evaluación disponibles pueden estar obsoletos. Esta revisión se
ha realizado para conocer el estado del arte sobre procesos de diseño,
construcción, validación y principales resultados obtenidos en estudios
empíricos acerca de los instrumentos de evaluación de la calidad de dichas
apps, todo ello a fin de identificar las principales dimensiones e indicadores
comunes. Se han llevado a cabo búsquedas en cuatro bases de datos de alto
impacto. Se concluye que es un tema de interés reciente y actual en la
literatura científica. De 11 documentos incluidos, se han hallado 97
indicadores organizados en 17 dimensiones. Sólo en dos de ellos se incluyeron
aspectos relacionados con la privacidad y la seguridad. En definitiva, se ha
configurado una lista significativa y actualizada que podrá ser la base para
construir un marco de evaluación que permita hacer un estudio integral de estas
apps, pues muchos de los instrumentos de evaluación no han sido diseñados
pensando en la población en general.
ABSTRACT
The download of the mobile
applications (apps) aimed at fostering healthy habits in the general population
has increased significantly in recent years. However, the majority of these
apps are not subject to quality regulation processes, and the available instruments
to assess the quality seem to be obsolete. This review has been made to know
the state of the art about the processes of design, construction, validation
and main results obtained in empirical studies about the instruments for
assessing the quality of said apps, all this in order to identify the main
dimensions and common indicators. Searches have been conducted in four
databases with high impact. It concludes that is an interest current topic in
scientific literature. From 11 documents which have been included, 17
dimensions and 97 indicators have been considered. Privacy and security-related
issues were only included in two documents. In short, it has been possible to
establish a significant and updated list that may be the basis for constructing
an evaluation framework that allows a comprehensive study of these apps,
considering that many of the assessment instruments have not been designed for
the general population.
PALABRAS CLAVES· KEYWORDS
Instrumento; evaluación; calidad; aplicación móvil;
hábitos saludables
Instrument; evaluation; quality; mobile application;
healthy habits
1. Introducción
Cada vez es mayor el uso cotidiano de las apps, pues
se consideran herramientas tecnológicas con numerosas posibilidades para
agilizar y controlar casi cualquier aspecto de nuestra vida.
En la última década, y en concreto desde finales del
año 2019, a causa de la COVID-19, se han incrementado exponencialmente sobre
todo el desarrollo y la publicación de apps sobre salud. Como señalan
Collado-Borrell et al. (2020), el inicio de la pandemia y sus efectos han sido
todo un punto de inflexión en el panorama de la mHealth. Este término, en
español mSalud (salud móvil), fue adoptado por la Organización Mundial de la
Salud (OMS, 2011, p.6) y engloba la “práctica médica y de salud pública
respaldada por dispositivos móviles, como teléfonos móviles, dispositivos de
monitoreo, asistentes digitales personales (PDA) y otros dispositivos
inalámbricos”.
Según Aitken and Nass (2021), actualmente existen más
de 350,000 apps relacionadas con la salud disponibles en todo el mundo. Y este
número no para de aumentar. Sin embargo, la gran mayoría no se basan en
evidencia científica ni han sido sometidas a procesos de regulación de calidad
y fiabilidad (Boudreaux et al., 2014; Duarte-Hueros et al., 2021;
Jake-Schoffman et al., 2017; Palacios et al., 2020). Como en su momento
reflexionaban Powell et al. (2014) en relación con la salud en general, el
creciente aumento del número de apps disponibles dificulta las tareas de
revisión y certificación que sería necesario llevar a cabo. Esto ha dado lugar
a una amplia desinformación entre la población y a la adopción de conductas
negativas para la salud al usar apps de baja calidad (BinDhim et al., 2015).
Si bien es cierto, como apuntan Lee and Cherner
(2015), que resulta prácticamente imposible crear un instrumento universal que
permita evaluar todas y cada una de las apps existentes debido a la diversidad
de temáticas y propósitos, así como a las continuas actualizaciones, también lo
es que muchas de las herramientas de evaluación disponibles (escalas, rúbricas,
listas de verificación, etc.) carecen de un enfoque multidimensional;
observándose demasiada heterogeneidad en los criterios de evaluación (Nouri et
al., 2018). En numerosas ocasiones, estos criterios son difíciles de
comprender, muy genéricos a veces e, incluso, demasiado específicos con
respecto a un aspecto de la salud en concreto (Stoyanov et al., 2015); o
simplemente, han quedado obsoletos para ayudar a la población en general a
seleccionar adecuadamente este tipo de tecnología. Todo ello hace que, como
recalcan Azad-Khaneghah et al. (2021), hoy en día sea tan complejo localizar un
instrumento de evaluación correcto como localizar una app idónea.
Con base en los argumentos anteriores, se ha llevado a
cabo una revisión de la literatura para conocer el estado del arte en relación
con los procesos de diseño, construcción, validación y principales resultados
recogidos en estudios empíricos sobre instrumentos de evaluación de la calidad
de apps orientadas a desarrollar hábitos saludables en la población en general.
El objetivo final de esta revisión ha sido identificar los instrumentos
utilizados en estudios previos, así como determinar las principales dimensiones
e indicadores comunes utilizados en los mismos.
2. Metodología
De acuerdo con el estudio de Grant and Booth (2009),
en el que se reconocen y describen hasta 14 tipos diferentes de revisiones de
literatura, la metodología seguida en esta investigación se ha desarrollado
siguiendo las pautas propias de la revisión sistemática, con un análisis de los
resultados de tipo bibliométrico seguido de un análisis cualitativo de los
estudios finalmente seleccionados.
El método utilizado ha seguido las directrices de la
Declaración PRISMA. De acuerdo con ella, durante el mes de marzo de 2022 se ha
llevado a cabo una consulta sistemática de las bases de datos bibliográficas de
relevancia en la investigación educativa: Web of Science y Scopus, y en las
bases de datos PubMed y Cochrane Library, por su especialización en Ciencias de
la Salud.
Los tópicos combinados en los que se ha centrado la
búsqueda han sido los siguientes: ((development OR validation) AND (instrument
OR tool OR method) AND (evaluation OR assessment) AND quality AND (“mobile
application” OR app) AND health*).
Como criterios de inclusión, se han tenido en cuenta:
(1) áreas temáticas de Ciencias Sociales, Ciencias de la Salud y Tecnología,
(2) apps relacionadas con la mHealth y (3) apps dirigidas a la población en
general.
No se han acotado las búsquedas con respecto al año de
publicación, tipo de documento, número de citas ni idioma para evitar excluir
posibles estudios afines.
De este modo, una vez cruzados los datos y eliminadas
las duplicidades del total de registros, se ha procedido a analizar el título,
el resumen y las palabras clave para confirmar aquellos que tenían que ver con
nuestro tema objeto de estudio, seleccionando los que describían el proceso de
investigación completo.
Como sistema de evaluación crítica de inclusión con
vistas a la selección final de documentos según la calidad metodológica, se ha
usado la herramienta MMAT de evaluación de métodos mixtos para revisiones
sistemáticas (Pluye et al., 2011) ya que se puede aplicar en investigaciones
basadas en cualquier tipo de diseño, dando lugar a una revisión integradora
completa (Coyne et al., 2018).
Las métricas de puntuación proporcionadas por MMAT
son: no clasificado (valor 0; falta de calidad), 25% de calidad, 50% de
calidad, 75% de calidad y 100%, es decir, mayor calidad metodológica del
estudio.
Después de la fase de extracción y evaluación con
MMAT, los datos han sido resumidos y sintetizados.
A continuación, se han extraído las dimensiones y los
indicadores de los estudios incluidos para identificar lo común a todos ellos.
Esta primera lista se ha refinado para eliminar las duplicidades.
Por último, a través de un nuevo análisis y depuración
de los ítems, se ha llevado a cabo una reorganización de las dimensiones y los
indicadores resultantes para confirmar que cada indicador estaba asociado a la
dimensión adecuada y esta, a su vez, quedaba claramente diferenciada del resto
por una descripción/explicación de lo que contenía.
3. Análisis y resultados
Se han identificado un total de 1,006 documentos. Tras
cruzar los datos y eliminar 368 duplicidades, se ha examinado el título, el
resumen y las palabras clave del resto (638 documentos). De estos, 42 han sido
excluidos al no cumplir con los criterios de elegibilidad fijados (indicados en
la Figura 1).
Los 596 documentos restantes han sido analizados a
texto completo para determinar su elegibilidad, lo que ha llevado a la
exclusión de 585 por las siguientes razones: (1) sin afinidad con la temática =
488; (2) no se especifica el instrumento o se utiliza una herramienta ya
elaborada y/o validada = 63; (3) apps no dirigidas a la población en general =
30; y (4) apps no relacionadas con la mHealth = 4. Este análisis ha sido
llevado a cabo de forma independiente por el autor C.D. y la autora A.D.,
resolviéndose cualquier discrepancia surgida mediante discusión y consenso.
Así pues, un total de 11 artículos se han incluido
finalmente para realizar el análisis documental detallado (Figura 1).
The mention of platforms as a novel advancement in
higher education may seem outdated due to the pandemic's reliance on
technology. Nowadays, it is challenging for educational institutions to
function without one.
The
use of digital technologies in higher education to promote the commodification
of education processes and practices has significant consequences. The
platformization of higher education is not a neutral shift, as platforms impact
institutions' values, culture, strategy, operations and outcome assessment.
These concerns about unrestricted platform use range from privacy issues to
changes in working conditions or profiles for teachers (Castañeda & Selwyn,
2018; Webber & Zheng, 2020). However, the potential impact on teaching and
learning cannot be ignored.
This
article explores the widespread use of platforms in universities, covering
their integration into various aspects such as administration and teaching. It
then examines stakeholder expectations for these platforms to transform higher
education while highlighting significant problems they present at institutional
and system levels. The dangers of platformization are summarized before
potential solutions are discussed to address these difficulties aligned with
the goals of higher education. Finally, lessons learned from this study are
presented as implications for future research and practice.
Diagrama de flujo PRISMA
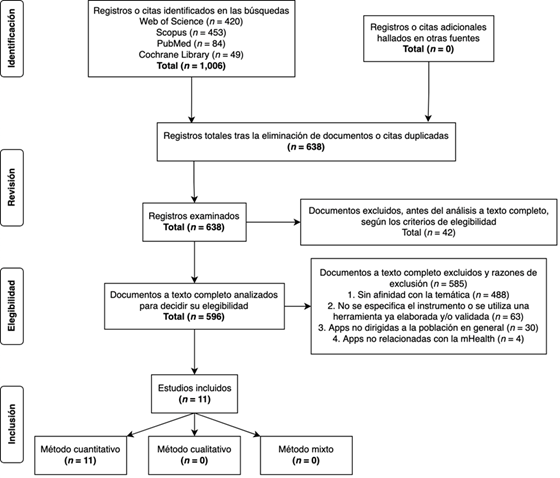
Fuente:
Basado en Moher et al. (2009)
En relación
con la calidad metodológica, los 11 artículos evaluados con MMAT han sido
incluidos ya que no ha habido ninguno con una calidad débil de sus componentes,
lo que ha dado lugar a una síntesis de estudios con una calidad alta-muy alta a
partir de la evidencia hallada (todos los estudios han cumplido con al menos el
75% de los criterios establecidos en la herramienta). De nuevo, el autor C.D. y
la autora A.D., de forma independiente, han sometido la lista final de los
artículos susceptibles de ser incluidos a esta evaluación de la calidad, y se
ha discutido cualquier desacuerdo para llegar a un consenso en la selección de
los mismos.
Los
resultados que se han obtenido de la evaluación crítica con MMAT para cada uno
de los documentos finalmente seleccionados se insertan en la siguiente tabla
(Tabla 1).
Tabla 1
Evaluación crítica de la calidad mediante MMAT (Pluye et al., 2011)
|
|
2. Cuantitativo controlado aleatorio |
4. Cuantitativo descriptivo |
Puntuación general de la calidad |
||||||||
|
Referencias |
2.1 |
2.2 |
2.3 |
2.4 |
4.1 |
4.2 |
4.3 |
4.4 |
|
||
|
Bardus
et al. (2020) |
|
|
|
|
Sí |
Sí |
Sí |
Sí |
**** |
||
|
Baumel
et al. (2017) |
|
|
|
|
Sí |
Sí |
Sí |
Sí |
**** |
||
|
Böhme
et al. (2019) |
|
|
|
|
No |
Sí |
Sí |
Sí |
*** |
||
|
Domnich
et al. (2016) |
|
|
|
|
Sí |
Sí |
Sí |
Sí |
**** |
||
|
Llorens-Vernet
and Miró (2020) |
|
|
|
|
Sí |
No |
Sí |
Sí |
*** |
||
|
Martín-Payo
et al. (2019) |
|
|
|
|
Sí |
Sí |
Sí |
Sí |
**** |
||
|
Messner
et al. (2020) |
|
|
|
|
Sí |
Sí |
Sí |
Sí |
**** |
||
|
Saliasi
et al. (2021) |
|
|
|
|
Sí |
Sí |
Sí |
Sí |
**** |
||
|
Stoyanov
et al. (2015) |
|
|
|
|
Sí |
Sí |
Sí |
Sí |
**** |
||
|
Stoyanov
et al. (2016) |
Sí |
No |
Sí |
Sí |
|
|
|
|
*** |
||
|
Terhorst
et al. (2020) |
|
|
|
|
Sí |
Sí |
Sí |
Sí |
**** |
||
|
*cumple con el 25% de los
criterios **cumple con el 50% de los
criterios ***cumple con el 75% de los
criterios ****cumple con el 100% de
los criterios n.c. (no clasificado) |
|||||||||||
Notas: Basado en Willis et al. (2019)
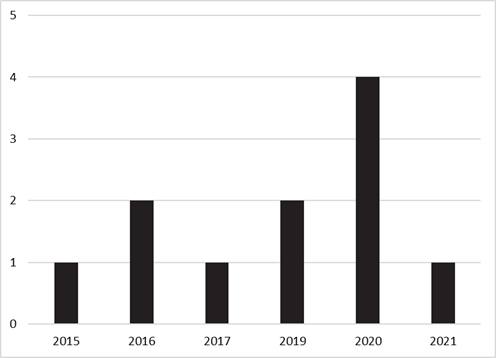
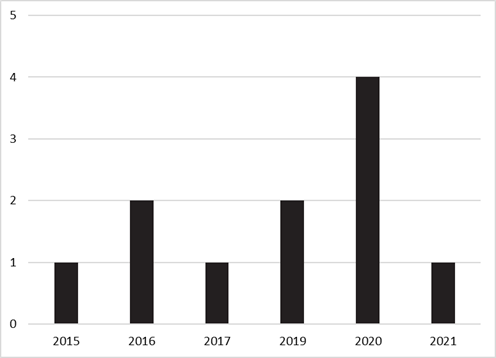
Los estudios
que se han incluido se sitúan geográficamente en seis países diferentes (Figura
2), publicándose la mayoría de ellos entre 2019 y 2021, y ampliándose el
periodo de publicación desde el año 2015 con el primer artículo elegible para
la revisión (Figura 3).
Países de origen de los
estudios incluidos

Figura 3
Año de publicación de los
estudios incluidos
En todos
los artículos se emplearon metodologías cuantitativas. En este sentido,
teniendo en cuenta los subdominios metodológicos, se han identificado diez con
un diseño cuantitativo descriptivo (Bardus et al., 2020; Baumel et al., 2017;
Böhme et al., 2019; Domnich et al., 2016; Llorens-Vernet &
Miró, 2020; Martín-Payo et al., 2019; Messner et al., 2020; Saliasi
et al., 2021; Stoyanov et al., 2015; Terhorst et al., 2020) y tan solo uno con
un diseño cuantitativo controlado aleatorio (Stoyanov et al., 2016).
Referente
a la evaluación con MMAT, de los estudios que utilizaron una metodología
centrada en un diseño cuantitativo descriptivo, se ha percibido en un artículo
una falta de justificación en la relevancia del tamaño de la muestra (Böhme
et al., 2019). No obstante, Böhme et al. (2019) reconocieron que el haber
utilizado exclusivamente apps alemanas
supuso una limitación en el estudio.
Por
otro lado, de nuevo dentro de este subdominio, ha habido un artículo que no ha
informado acerca de las razones por las que ciertos sujetos elegibles
decidieron no participar tanto en la primera como en la segunda ronda del
método Delphi (Llorens-Vernet & Miró, 2020). Aun así, comentaron que
las diferencias entre las rondas fueron mínimas a pesar de que no todos los
sujetos de la primera ronda (n = 42) participaron en la siguiente (n = 24), por
lo que el número de sujetos participantes en cada ronda fue apropiado para los
objetivos propuestos.
El
único artículo de corte cuantitativo controlado aleatorio no ha proporcionado
suficientes detalles sobre el ocultamiento de la asignación o el cegamiento
posterior a la aleatorización (Stoyanov et al., 2016). Según Schulz and Grimes
(2002), el ocultamiento de la asignación es un método utilizado en los ensayos
controlados aleatorios para evitar el sesgo de selección, así como para
proteger una secuencia de asignación antes y hasta el propio momento de la
asignación. En cambio, con el cegamiento se mantienen a los sujetos
participantes y/o a las personas responsables del estudio ajenas a la
intervención asignada para evitar cualquier posible influencia, protegiéndose
de esta manera la secuencia después de la asignación.
Atendiendo
al objetivo de los estudios, el desarrollo de un instrumento, una herramienta o
un método de evaluación únicamente se ha abordado en dos artículos, en los
cuales se ha incluido el proceso de validación. Baumel et al. (2017)
presentaron la herramienta Enlight,
que es un conjunto de escalas para evaluar la calidad de los programas
pertenecientes a la salud electrónica o cibersalud. Por su parte, Stoyanov et
al. (2015) dieron a conocer la multidimensional Mobile App Rating Scale
(MARS) para determinar la calidad de las apps
de salud.
En
cuanto al mecanismo de medición utilizado en dichas escalas, en ambos estudios
se ha construido una escala tipo Likert de cinco puntos.
Lo
más frecuente ha sido la traducción, adaptación y validación a otro idioma de
un instrumento, una herramienta o un método de evaluación previamente
desarrollado, en concreto la escala MARS diseñada por Stoyanov et al. (2015).
Así ha sido en cinco de los artículos consultados: Bardus et al. (2020),
Domnich et al. (2016), Martín-Payo et al. (2019), Messner et al. (2020) y
Saliasi et al. (2021). Asimismo, el desarrollo y/o la validación de una versión
alternativa se ha llevado a cabo en dos artículos (Böhme et al., 2019; Stoyanov
et al., 2016).
Los
artículos restantes se han centrado en el proceso de validación de un
instrumento, una herramienta o un método de evaluación construido con
anterioridad. Por un lado, Llorens-Vernet and Miró (2020) validaron la Mobile App Development and Assessment Guide (MAG), una guía inédita
basada en una checklist o lista de
verificación para ayudar a diseñar, desarrollar y analizar, en términos de
calidad, las apps propias de la mHealth. Y, por otro lado, Terhorst et
al. (2020) se ocuparon de la evaluación psicométrica de la escala incluida en
el citado estudio de Stoyanov et al. (2015).
La
relación de artículos finalmente incluidos puede consultarse en la Tabla 2, en
la que se ofrece información detallada en relación con la autoría, año de
publicación, diseño, objetivos, principales resultados y puntajes MMAT.
Tabla 2
Resumen de los estudios incluidos
|
Autoría |
Año |
Diseño |
Objetivo(s) |
Principales resultados |
Punt. MMAT |
|
Stoyanov et al. |
2015 |
Cuantitativo descriptivo |
Desarrollar una escala de
evaluación (MARS) |
Escala MARS. Excelente
consistencia interna: α = .90 (también altos valores en todas las
dimensiones). Excelente fiabilidad entre evaluadores: CCI = .79 |
100%
(****) |
|
Domnich et al. |
2016 |
Cuantitativo descriptivo |
Traducir, adaptar y validar
al italiano la escala MARS |
Escala MARS-It. Excelente
consistencia interna: α = .90 y .91 (ambos evaluadores). Excelente
fiabilidad entre evaluadores: CCI = .96 |
100%
(****) |
|
Stoyanov et al. |
2016 |
Cuantitativo controlado
aleatorio |
Desarrollar y validar la
versión de usuario de la escala MARS (uMARS) |
Escala uMARS. Excelente
consistencia interna: α = .90 (también altos valores en todas las
dimensiones). La puntuación total y las dimensiones tuvieron unos buenos
niveles de fiabilidad entre evaluadores test-retest durante los periodos de
uno a dos meses y tres meses: CCI = .66 y .70 |
75%(a)
(***) |
|
Baumel et al. |
2017 |
Cuantitativo descriptivo |
Desarrollar y validar una
herramienta de evaluación (Enlight) |
Herramienta Enlight. Excelente consistencia
interna: α = rango .83-.90 (también altos valores en todas las
dimensiones). Excelente fiabilidad entre evaluadores: CCI = rango .77-.98 |
100%
(****) |
|
Böhme et al. |
2019 |
Cuantitativo descriptivo |
Desarrollar una herramienta
de evaluación basada en la escala MARS |
Herramienta basada en la
escala MARS. Validación/Evaluación psicométrica n.p. |
75%(b)
(**) |
|
Martín-Payo et al. |
2019 |
Cuantitativo descriptivo |
Traducir, adaptar y validar
al español la escala MARS |
Escala MARS-Sp. Alta
consistencia interna: α = >.77 (independientemente del evaluador).
Alta fiabilidad entre evaluadores: CCI = >.76. También altos valores en la
correlación de las dimensiones |
100%
(****) |
|
Bardus et al. |
2020 |
Cuantitativo descriptivo |
Traducir, adaptar y validar
al árabe la escala MARS |
Escala MARS-Ar. Buena consistencia
interna: α = .96 (compromiso), .94 (estética), .81 (calidad de la
información) y .71 (funcionalidad). Buena fiabilidad entre evaluadores: CCI =
.83. Escala altamente alineada con la versión original |
100%
(****) |
|
Llorens-Vernet and Miró |
2020 |
Cuantitativo descriptivo |
Validar la guía MAG |
Se establecieron un total
de 48 criterios finales (método Delphi). Usabilidad, privacidad y seguridad
fueron las dimensiones que incluyeron los criterios más relevantes |
75%(c)
(***) |
|
Messner et al. |
2020 |
Cuantitativo descriptivo |
Traducir, adaptar y validar
al alemán la escala MARS |
Escala MARS-G. Buena
consistencia interna: Omega = rango .72-.91. Alta fiabilidad entre evaluadores:
CCI = .83. También altos valores en la correlación de las dimensiones. Escala
excelentemente alineada con la versión original |
100%
(****) |
|
Terhorst et al. |
2020 |
Cuantitativo descriptivo |
Validar la escala MARS |
El AFC generó un modelo
bifactorial con un factor general y un factor para cada dimensión.
Buena/excelente consistencia interna: Omega = rango .79-.93. Alta fiabilidad
entre evaluadores: CCI = .82. También altos valores en la correlación de MARS
con la herramienta Enlight |
100%
(****) |
|
Saliasi et al. |
2021 |
Cuantitativo descriptivo |
Traducir, adaptar y validar
al francés la escala MARS |
Escala MARS-F. Aceptable
consistencia interna: Omega = .79 (compromiso), .79 (funcionalidad), .78
(estética) y .61 (calidad de la información). También altos valores en la
correlación de las dimensiones. Escala bien alineada con la versión original |
100%
(****) |
|
Notas: (a) No se especifica el método de ocultamiento de la asignación
o el cegamiento posterior a la aleatorización. (b) Se percibe falta de justificación en la relevancia
del tamaño de la muestra (prueba piloto). (c) No se explican las razones por las que ciertos sujetos
elegibles decidieron no participar en las rondas del método Delphi. |
|||||
|
AFC –
Análisis factorial confirmatorio. |
|||||
CCI – Coeficiente de correlación intraclase.
MAG – Mobile App Development and Assessment Guide (guía de evaluación y desarrollo de apps).
MARS – Mobile App Rating Scale (escala de calificación de apps).
MMAT – Mixed Methods Appraisal Tool (herramienta de evaluación de métodos
mixtos).
n.p. – No proporcionado.
A continuación,
se han extraído todas las dimensiones e indicadores utilizados en dichos
artículos, resultando en 59 dimensiones y 282 indicadores en total. Tras
eliminar duplicidades y fusionar dimensiones e indicadores similares, la lista
final ha quedado conformada por un total de 97 indicadores agrupados en 17
dimensiones (tabla 3). Para delimitar de forma clara la especificidad de cada
dimensión, se ha realizado una explicación/descripción detallada de lo que
contenían. Esta información no se ha incluido en este documento por motivos de
espacio, pero puede solicitarse a las personas responsables del estudio.
Tabla 3
Relación de dimensiones consideradas
|
Dimensiones |
|
|
1.
Compromiso/Participación |
10. Soporte
técnico y actualizaciones |
|
2.
Funcionalidad (técnica/tecnología) |
11.
Psicoterapia |
|
3.
Funcionalidad (usabilidad) |
12.
Psicoterapia (usabilidad) |
|
4.
Funcionalidad (accesibilidad) |
13.
Seguridad de uso |
|
5.
Estética/Diseño visual |
14. Calidad/Evaluación
subjetiva |
|
6.
Información |
15.
Calidad/Evaluación subjetiva (predisposición) |
|
7.
Información (base científica) |
16.
Persuasión terapéutica |
|
8.
Información (ética) |
17.
Alianza terapéutica |
|
9. Privacidad/Seguridad
de datos |
|
4. Discusión
En
primer lugar, con respecto al análisis bibliométrico realizado, se ha observado
que la fecha de publicación de documentos relacionados con la temática objeto
de estudio se inicia en 2015; hecho que demuestra que la evaluación de apps del ámbito de la mHealth es
un tema de interés reciente en lo que a la literatura científica se refiere, coincidiendo
con los resultados obtenidos en otros estudios (Azad-Khaneghah et al., 2021;
Nouri et al., 2018). Alemania y Australia son los países que concentran la
mayor parte de las investigaciones sobre el tema.
En
consonancia con estudios como el de Azad-Khaneghah et al. (2021), resulta
llamativo el gran número de trabajos hallados que se refieren a la escala MARS
al ser la primera herramienta para medir la calidad de las apps de salud. Si bien se ha adaptado a diferentes idiomas y
versiones, y ha adquirido un evidente reconocimiento en la comunidad científica
(Bardus et al., 2020; Böhme et al., 2019; Domnich et al., 2016;
Martín-Payo et al., 2019; Messner et al., 2020; Saliasi et al., 2021;
Stoyanov et al., 2016), se evidencian algunas carencias, pues no se incluyen
dimensiones ni indicadores relacionados con temas de privacidad y seguridad;
resultados a los que también llegaron Hensher et al. (2021) y Jeminiwa et al.
(2019).
Según
los resultados del estudio sistemático realizado por Duarte-Hueros et al.
(2021) sobre las iniciativas españolas acreditadoras de calidad y sus procesos
de regulación en apps del campo de la
salud, se ha observado que los indicadores, los criterios y las recomendaciones
contenidas en tales iniciativas tienen similitudes relevantes con esta
revisión. Buena parte de las recomendaciones del distintivo AppSaludable
y de los criterios del servicio de certificación Acreditació FTSS aparecen entre los resultados que aquí se han
presentado. Aunque existen algunas coincidencias, la terminología empleada es,
en líneas generales, distinta.
Además,
algo significativo en estas iniciativas es que se valoran variables relacionadas
con la privacidad y la seguridad; dos dimensiones que, en este caso y a
diferencia de la mayoría de los instrumentos de evaluación analizados, sí han
sido consideradas y convenientemente descritas en el presente estudio.
5. Conclusiones
De
acuerdo con los datos obtenidos a partir de la herramienta MMAT en relación con
el diseño metodológico seguido en los estudios analizados, se concluye que la
investigación en esta área se ha abordado en su mayor parte desde una
perspectiva cuantitativa descriptiva, mostrando una calidad metodológica
notable: los 11 artículos han cumplido con al menos el 75% de los criterios
contemplados en la herramienta.
A
partir de las distintas dimensiones e indicadores comunes identificados en los
estudios analizados, y de la información contrastada con otros documentos, esta
investigación supone el punto de partida para la construcción de un marco de
evaluación de la calidad de apps;
máxime considerando que las escalas/instrumentos disponibles en la actualidad
no se orientan a la evaluación de apps para
la población en general (Azad-Khaneghah et al., 2021) ni a apps que fomenten/desarrollen hábitos saludables.
En ninguno de los estudios se incluyen
descripciones/explicaciones claras de cada dimensión. Al respecto, esta investigación
es novedosa, ya que se ha hecho un esfuerzo para hacerlas más comprensibles y
mejorar su concordancia con el conjunto de indicadores asociados a cada una de
ellas.
En
cuanto a las limitaciones del estudio, hay que tener presente la naturaleza cambiante
y dinámica de la tecnología, por lo que se recomienda revisar con cierta
frecuencia las dimensiones y los indicadores hallados. En este sentido, a pesar
de haber consultado bases de datos de alto impacto científico (Web of
Science, Scopus, PubMed y Cochrane Library), se han
obviado indexaciones en otras bases de datos donde podría ubicarse literatura
valiosa sobre el tema objeto de estudio.
Con
perspectivas de futuro, se sugiere el desarrollo de estudios con diseños metodológicos controlados que, a su
vez, proporcionen una explicación en profundidad de cada dimensión e
indicadores, además de incluir categorías relacionadas con la privacidad y la
seguridad como parte de una evaluación integral de cualquier app.
6. Financiación
Este
trabajo ha sido apoyado por la Estrategia de Política de Investigación y
Transferencia de la Universidad de Huelva (ayudas predoctorales de Personal
Investigador en Formación, 2020).
Systematic review of instruments that assess the
quality of mobile health applications
1. Introduction
The daily use of apps is increasing, as they are seen
as technological tools with numerous possibilities to streamline and control
almost any aspect of our lives.
In the last decade, and specifically since the end of
2019 due to COVID-19, the development and release of health apps in particular
has increased exponentially. As Collado-Borrel et al. (2020) point out, the
onset of the pandemic and its effects have been a turning point in the mHealth
landscape. This term, mHealth (mobile health), was adopted by the World Health
Organisation (WHO, 2011, p.6) and encompasses "medical and public health
practice supported by mobile devices, such as mobile phones, monitoring devices,
personal digital assistants (PDAs) and other wireless devices".
According to Aitken and Nass (2021), there are
currently more than 350,000 health-related apps available worldwide. And this
number keeps growing. However, the vast majority are not based on scientific
evidence, nor have they been subject to quality and reliability regulation
processes (Boudreaux et al., 2014; Duarte-Hueros et al., 2021; Jake-Schoffman
et al., 2017; Palacios et al., 2020). As reflected by Powell et al. (2014) in
relation to health in general, the increasing number of apps available makes it
more difficult to carry out the necessary review and certification procedures.
This has led to widespread misinformation among the population and the adoption
of behaviours that have a negative effective on health due to using low-quality
apps (BinDhim et al., 2015).
While it is true, as Lee and Cherner (2015) point out,
that it is practically impossible to create a universal instrument to evaluate
each and every app that exists due to the diversity of topics and purposes that
they cover, as well as the continuous updates, it is also true that many of the
available evaluation tools (scales, rubrics, checklists, etc.) lack a
multidimensional approach; too much heterogeneity is found in the evaluation
criteria (Nouri et al., 2018). These criteria are often difficult to
understand, are sometimes too generic or are even too specific to a particular
aspect of health (Stoyanov et al., 2015), or they have simply become obsolete
in helping the general population to select this type of technology
appropriately. All of this means that, as Azad-Khaneghah et al. (2021)
emphasise, nowadays it is as difficult to find the right assessment tool as it
is to find a suitable app.
Based on the above arguments, a literature review has
been carried out to determine the state of the art in relation to the processes
of design, construction and validation, as well as the main results collected
in empirical studies carried out on the instruments used to assess the quality
of apps which are aimed at developing healthy habits in the general population.
The overall aim of this review has been to identify the instruments used in
previous studies, as well as to determine the main common dimensions and
indicators used in these studies.
2. Methodology
In accordance with the study by Grant and Booth
(2009), which recognises and describes up to 14 different types of literature
reviews, the methodology followed in this research has been developed following
the guidelines of the systematic review, with a bibliometric analysis of the
results followed by a qualitative analysis of the studies finally selected.
The method used has followed the guidelines of the
PRISMA Statement. Accordingly, during the month of March 2022, a systematic
consultation of important bibliographic databases in educational research was
carried out: Web of Science and Scopus, and in the PubMed and Cochrane Library
databases, for their specialisation in Health Sciences.
The topics on which the search focused were as
follows: ((development OR validation) AND (instrument OR tool OR method) AND
(evaluation OR assessment) AND quality AND (“mobile application” OR app) AND
health*).
For the inclusion criteria, the following were
considered: (1) thematic areas of Social Sciences, Health Sciences and
Technology, (2) apps related to mHealth and (3) apps aimed at the general
public.
Searches have not been narrowed down with respect to
year of publication, type of paper, number of citations or language to avoid
excluding possible related studies.
Thus, after cross-checking the data and eliminating
duplicates from the total number of records, we proceeded to analyse the title,
abstract and keywords to confirm those that were related to our topic of study,
selecting those that described the entire research process.
As a critical inclusion assessment system for the
final selection of papers according to methodological quality, the MMAT (mixed
methods appraisal tool) for systematic reviews (Pluye et al., 2011) has been
used, as it can be applied to research based on any type of design, resulting
in a comprehensive review (Coyne et al., 2018).
The scoring metrics provided by MMAT are: not
classified (value 0; lack of quality), 25% quality, 50% quality, 75% quality
and 100%, i.e., the highest methodological quality of the study.
After the extraction and evaluation phase with MMAT,
the data were summarised and synthesised.
The dimensions and indicators of the included studies
have been extracted below to identify commonalities. This initial list has been
refined to eliminate duplication.
Finally, through a re-analysis and refinement of the
items, a reorganisation of the dimensions and the resulting indicators was
carried out to confirm that each indicator was associated with the appropriate
dimension and that this, in turn, was clearly differentiated from the rest by a
description/explanation of what it contained.´
3. Analysis and
results
A total of 1006 documents were identified. After
cross-checking the data and eliminating 368 duplicates, the title, abstract and
keywords of the remaining 638 documents were examined. Of these, 42 were
excluded as they did not meet the eligibility criteria (shown in figure 1).
The remaining 596 documents were analysed in full to
determine their eligibility, leading to the exclusion of 585 for the following
reasons: (1) no thematic affinity = 488; (2) no instrument specified or a tool
that has already been developed and/or validated is used = 63; (3) apps not
aimed at the general population = 30; and (4) apps not related to mHealth = 4.
This analysis was carried out independently by author C.D. and author A.D.,
with any discrepancies resolved through discussion and consensus.
Thus, a total of 11 articles were finally included for
the detailed documentary analysis (Figure 1).
Figure 1
PRISMA flow diagram
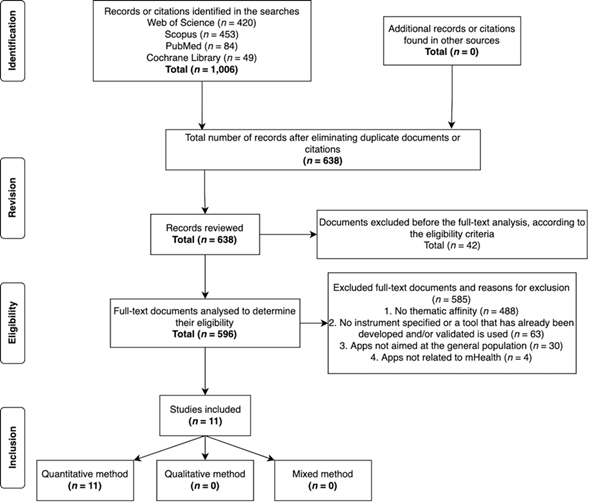
Source: Based on
Moher et al. (2009)
In relation to methodological quality, all 11 articles
assessed with MMAT have been included as there were none with poor-quality components,
resulting in a synthesis of studies with a high/very high quality based on the
evidence found (all studies met at least 75% of the criteria set out in the
tool). Again, author C.D. and author A.D. independently submitted the final
list of articles for inclusion in this quality assessment, and any
disagreements were discussed in order to reach a consensus on the selection of
articles.
The results obtained from the critical assessment with
MMAT for each of the documents finally selected are inserted in Table 1 below.
Table 1
Critical quality assessment using MMAT (Pluye et al.,
2011)
|
|
2.
Quantitative randomised controlled |
4.
Descriptive quantitative |
General
quality score |
||||||||
|
References |
2.1 |
2.2 |
2.3 |
2.4 |
4.1 |
4.2 |
4.3 |
4.4 |
|
||
|
Bardus
et al. (2020) |
|
|
|
|
Yes |
Yes |
Yes |
Yes |
**** |
||
|
Baumel
et al. (2017) |
|
|
|
|
Yes |
Yes |
Yes |
Yes |
**** |
||
|
Böhme
et al. (2019) |
|
|
|
|
No |
Yes |
Yes |
Yes |
*** |
||
|
Domnich
et al. (2016) |
|
|
|
|
Yes |
Yes |
Yes |
Yes |
**** |
||
|
Llorens-Vernet
and Miró (2020) |
|
|
|
|
Yes |
No |
Yes |
Yes |
*** |
||
|
Martín-Payo
et al. (2019) |
|
|
|
|
Yes |
Yes |
Yes |
Yes |
**** |
||
|
Messner
et al. (2020) |
|
|
|
|
Yes |
Yes |
Yes |
Yes |
**** |
||
|
Saliasi
et al. (2021) |
|
|
|
|
Yes |
Yes |
Yes |
Yes |
**** |
||
|
Stoyanov
et al. (2015) |
|
|
|
|
Yes |
Yes |
Yes |
Yes |
**** |
||
|
Stoyanov
et al. (2016) |
Yes |
No |
Yes |
Yes |
|
|
|
|
*** |
||
|
Terhorst
et al. (2020) |
|
|
|
|
Yes |
Yes |
Yes |
Yes |
**** |
||
|
*meets 25% of the criteria ** meets 50% of the criteria *** meets 75% of the criteria **** meets 100% of the criteria n.c. (not classified) |
|
||||||||||
Notes: Based on Willis
et al. (2019)
The studies included are geographically located in six
different countries (Figure 2), with most of them published between 2019 and 2021,
and with the publication period starting from 2015 with the first article
eligible for review (Figure 3).
Figure 2
Country of origin of the studies included
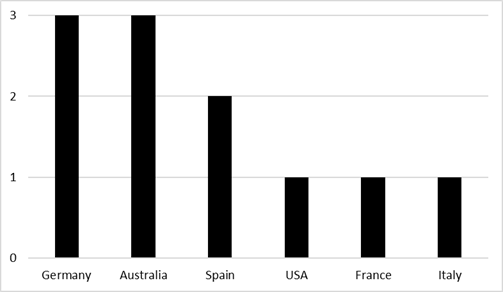
Figure 3
Year of publication of the studies included
Quantitative methodologies were used in all of the
articles. In this sense, taking into account the methodological subdomains, ten
have been identified with a descriptive quantitative design (Bardus et al.,
2020; Baumel et al., 2017; Böhme et al., 2019; Domnich et al, 2016;
Llorens-Vernet & Miró, 2020; Martín-Payo et al., 2019; Messner et al.,
2020; Saliasi et al., 2021; Stoyanov et al., 2015; Terhorst et al., 2020) and
only one with a quantitative randomised controlled design (Stoyanov et al.,
2016).
Regarding the assessment with MMAT, of the studies that
used a methodology focusing on a descriptive quantitative design, a lack of
justification of the relevance of the sample size has been perceived in one
article (Böhme et al., 2019). However, Böhme et al. (2019) acknowledged that
using only German apps was a limitation of the study.
Furthermore, again within this subdomain, one article
didn’t report on the reasons why certain eligible subjects decided to not
participate in both the first and second rounds of the Delphi method
(Llorens-Vernet & Miró, 2020). However, they reported that the differences
between rounds were minimal and despite the fact that not all subjects from the
first round (n = 42) participated in the following round (n = 24), the number
of subjects participating in each round was appropriate for the proposed
objectives.
The only quantitative randomised controlled article
has not provided sufficient detail on allocation concealment or
post-randomisation blinding (Stoyanov et al., 2016). According to Schulz and
Grimes (2002), allocation concealment is a method used in randomised controlled
trials to avoid selection bias, as well as to protect an allocation sequence
before and up to the point of allocation. Blinding, on the other hand, keeps
the participating subjects and/or the persons responsible for the study away
from the assigned intervention to avoid any possible influence, thus protecting
the post-assignment sequence.
In view of the objective of the studies, the
development of an assessment instrument, tool or method has only been addressed
in two articles, in which the validation process has been included. Baumel et
al. (2017) presented the Enlight
tool, which is a set of scales for assessing the quality of e-health
programmes. Meanwhile, Stoyanov et al. (2015) unveiled the multidimensional
Mobile App Rating Scale (MARS) to determine the quality of health apps.
As for the measurement mechanism used in these scales,
a five-point Likert-type scale was applied in both studies.
In most cases, a previously developed instrument, tool
or assessment method was translated, adapted and validated in another language,
specifically the MARS scale designed by Stoyanov et al. (2015). This was the
case in five of the articles consulted: Bardus et al. (2020), Domnich et al. (2016),
Martín-Payo et al. (2019), Messner et al. (2020) and Saliasi
et al. (2021). Furthermore, the development and/or validation of an alternative
version was carried out in two articles (Böhme et al., 2019; Stoyanov et al.,
2016).
The remaining articles focused on the validation process
of a previously constructed assessment instrument, tool or method. On the one
hand, Llorens-Vernet and Miró (2020) validated the Mobile App Development and
Assessment Guide (MAG), an unpublished guide based on a checklist to help
design, develop and analyse mHealth apps in terms of quality. On the other
hand, Terhorst et al. (2020) focused on the psychometric evaluation of the
scale included in the aforementioned study by Stoyanov et al. (2015).
The list of articles finally included can be found in
Table 2 below, which provides detailed information regarding authorship, year
of publication, design, objectives, main results and MMAT scores.
Table 2
Summary of the studies included
|
Authorship |
Year |
Design |
Objective(s) |
Main results |
MMAT score |
|
Stoyanov et al. |
2015 |
Descriptive quantitative |
Development of an
assessment scale (MARS) |
MARS scale. Excellent
internal consistency: α = .90 (also high values in all dimensions). Excellent
inter-rater reliability: ICC = .79 |
100% (****) |
|
Domnich et al. |
2016 |
Descriptive quantitative |
Translating, adapting and
validating the MARS scale in Italian |
MARS-It scale. Excellent
internal consistency: α = .90 and .91 (both raters). Excellent inter-rater
reliability: ICC = .96 |
100% (****) |
|
Stoyanov et al. |
2016 |
Quantitative randomised
controlled |
Developing and validating
the user version of the MARS scale (uMARS) |
uMARS scale. Excellent
internal consistency: α = .90 (also high values in all dimensions). The
total score and the dimensions had good levels of inter-rater test-retest
reliability during the one- to two-month and three-month periods: ICC = .66
and .70 |
75%(a) (***) |
|
Baumel et al. |
2017 |
Descriptive quantitative |
Developing and validating
an assessment tool (Enlight) |
Enlight Tool. Excellent internal
consistency: α = range .83-.90 (also high values in all dimensions).
Excellent inter-rater reliability: ICC = range .77-.98 |
100% (****) |
|
Böhme et al. |
2019 |
Descriptive quantitative |
Developing an assessment
tool based on the MARS scale |
Instrument based on the
MARS scale. Psychometric evaluation/validation n.p. |
75%(b) (**) |
|
Martín-Payo et al. |
2019 |
Descriptive quantitative |
Translating, adapting and
validating the MARS scale in Spanish |
MARS-Sp scale. High
internal consistency: α = >.77 (independent of rater). High
inter-rater reliability: ICC = >.76. High values in the correlation of the
dimensions |
100% (****) |
|
Bardus et al. |
2020 |
Descriptive quantitative |
Translating, adapting and
validating the MARS scale in Arabic |
MARS-Ar scale. Good
internal consistency: α = .96 (engagement), .94 (aesthetics), .81
(quality of information) and .71 (functionality). Good inter-rater
reliability: ICC =.83. Scale highly aligned with the original version |
100% (****) |
|
Llorens-Vernet and Miró |
2020 |
Descriptive quantitative |
Validating the MAG guide |
A total of 48 final
criteria were established (Delphi method). Usability, privacy and security
were the dimensions that included the most relevant criteria |
75%(c) (***) |
|
Messner et al. |
2020 |
Descriptive quantitative |
Translating, adapting and
validating the MARS scale in German |
MARS-G scale. Good internal
consistency: Omega = range .72-.91. High inter-rater reliability: ICC =.83.
High values in the correlation of the dimensions. Scale excellently aligned
with the original version |
100% (****) |
|
Terhorst et al. |
2020 |
Descriptive quantitative |
Validating the MARS guide |
The CFA generated a bifactorial
model with a general factor and a factor for each dimension. Good/excellent
internal consistency: Omega = range .79-.93. High inter-rater reliability:
ICC =.82. High values in the correlation of MARS with the Enlight tool |
100% (****) |
|
Saliasi et al. |
2021 |
Descriptive quantitative |
Translating, adapting and
validating the MARS scale in French |
MARS-F scale. Acceptable
internal consistency: Omega = .79 (engagement), .79 (functionality), .78
(aesthetics) and .61 (quality of information). High values in the correlation
of the dimensions. Scale well aligned with the original version |
100% (****) |
|
Notes: (a) The method of allocation concealment or
post-randomisation blinding is not specified. (b) There is a perceived lack of justification for
the relevance of the sample size (pilot test). (c) The reasons why certain eligible subjects
decided to not participate in the Delphi rounds are not explained. |
|||||
|
CFA - Confirmatory factor analysis. ICC - Intraclass correlation coefficient. MAG – Mobile App Development and Assessment
Guide. MARS - Mobile App Rating Scale. MMAT - Mixed Methods Appraisal Tool. n.p. - Not provided. |
|||||
All dimensions and indicators used in these articles
were then extracted, resulting in 59 dimensions and 282 indicators in total.
After eliminating duplicates and merging similar dimensions and indicators, the
final list was made up of a total of 97 indicators grouped into 17 dimensions
(Table 3). In order to clearly delimit
the specificity of each dimension, a detailed explanation/description of what
they contain has been made. This information hasn’t been included in this
document due to lack of space, but it can be obtained from the people in charge
of the study.
Table 3
List of dimensions considered
|
Dimensions |
|
|
1. Engagement/Participation |
10. Technical support and updates |
|
2. Functionality (technical/technology) |
11. Psychotherapy |
|
3. Functionality (usability) |
12. Psychotherapy (usability) |
|
4. Functionality (accessibility) |
13. Safety of use |
|
5. Aesthetic/ Visual design |
14. Quality/Subjective assessment |
|
6. Information |
15. Quality/Subjective assessment
(predisposition) |
|
7. Information (scientific basis) |
16. Therapeutic persuasion |
|
8. Information (ethics) |
17. Therapeutic alliance |
|
9. Privacy/Data security |
|
4. Discussion
Firstly, regarding the bibliometric analysis carried
out, it has been observed that the date of publication of documents related to
the topic being studied began in 2015; this shows that the evaluation of apps
in the field of mHealth is a recent topic of interest in terms of scientific
literature, coinciding with the results obtained in other studies
(Azad-Khaneghah et al., 2021; Nouri et al., 2018). Germany and Australia are
the countries where the majority of the studies on this topic have been carried
out.
In line with studies such as Azad-Khaneghah et al.
(2021), it is striking to note the large number of papers that refer to the
MARS scale as the first tool to measure the quality of health apps. Although it
has been adapted into different languages and versions, and has gained obvious
recognition in the scientific community (Bardus et al., 2020; Böhme et al.,
2019; Domnich et al., 2016; Martín-Payo et al., 2019; Messner et al.,
2020; Saliasi et al., 2021; Stoyanov et al., 2016), there are some shortcomings,
as no dimensions or indicators related to privacy and security issues are
included; conclusions that were also reached by Hensher et al. (2021) and
Jeminiwa et al. (2019).
According to the results of the systematic study
conducted by Duarte-Hueros et al. (2021) on the Spanish quality accreditation
initiatives and their regulatory processes in health apps, it has been observed
that the indicators, criteria and recommendations contained in such initiatives
have relevant similarities with this review.
Many of the recommendations of the AppSaludable
label and the criteria of the Acreditació
FTSS certification service appear among the results presented here.
Although there are some overlaps, the terminology used is broadly different.
Furthermore, a significant aspect of these initiatives
is that variables related to privacy and security are assessed; two dimensions
that, in this case and unlike most of the evaluation instruments analysed, have
been considered and conveniently described in this study.
5. Conclusions
According to the data obtained from the MMAT tool in
relation to the methodological design followed in the studies analysed, it can be
concluded that research in this area has mostly been approached from a
descriptive quantitative perspective, showing a noteworthy methodological
quality: the 11 articles met at least 75% of the criteria set out in the tool.
Based on the different dimensions and common
indicators identified in the studies analysed, and the information contrasted
with other documents, this research is the starting point for the construction
of a framework for the evaluation of app quality, especially considering that
the scales/instruments currently available are not oriented towards the
evaluation of apps for the general population (Azad-Khaneghah et al., 2021) or
apps that promote/develop healthy habits.
None of the studies include clear
descriptions/explanations of each dimension. In this respect, this research is
novel, as an effort has been made to make them more comprehensible and to
improve their alignment with the related set of indicators.
In terms of limitations of the study, the changing and
dynamic nature of technology should be borne in mind, and it is therefore
recommended that the dimensions and indicators identified be reviewed at
regular intervals. In this sense, despite having consulted databases of high
scientific impact (Web of Science, Scopus, PubMed and Cochrane Library), we
have avoided indexing in other databases where valuable literature on the
subject under study could be found.
With a view to the future, it is suggested that
studies with controlled methodological designs should be developed which, in
turn, could provide an in-depth explanation of each dimension and indicator, as
well as including categories related to privacy and security as part of a
comprehensive assessment of any app.
6. Funding
This work has been supported by the Research and Transfer
Policy Strategy of the University of Huelva (predoctoral grants for Research
Staff in Training, 2020).
References
Aitken, M. & Nass,
D. (2021). Digital Health Trends 2021: Innovation, evidence, regulation, and
adoption. IQVIA Institute for Human Data Science. https://bit.ly/33sHF9k
Azad-Khaneghah, P., Neubauer,
N., Cruz, A. M. & Liu, L. (2021). Mobile health app usability and quality
rating scales: a systematic review. Disability and Rehabilitation: Assistive
Technology, 16(7), 712-721. https://doi.org/10.1080/17483107.2019.1701103
Bardus, M., Awada, N.,
Ghandour, L. A., Fares, E., Gherbal, T., Al-Zanati, T. & Stoyanov, S. R.
(2020). The Arabic Version of the Mobile App Rating Scale: Development and
Validation Study. JMIR MHealth Uhealth, 8(3), e16965. https://doi.org/10.2196/16956
Baumel, A., Mathur, N., Kane,
J. M. & Muench, F. (2017). Enlight: A Comprehensive Quality and Therapeutic
Potential Evaluation Tool for Mobile and Web-Based eHealth Interventions. Journal
of Medical Internet Research, 19(3), e82. https://doi.org/10.2196/jmir.7270
BinDhim, N. F., Hawkey, A.
& Trevena, L. (2015). A Systematic Review of Quality Assessment Methods for
Smartphone Health Apps. Telemedicine and e-Health, 21(2), 97-104. https://doi.org/10.1089/tmj.2014.0088
Böhme, C., von Osthoff,
M. B., Frey, K. & Hübner, J. (2019). Development of a Rating Tool for
Mobile Cancer Apps: Information Analysis and Formal and Content-Related
Evaluation of Selected Cancer Apps. Journal of Cancer Education, 34(1),
105-110. https://doi.org/10.1007/s13187-017-1273-9
Boudreaux, E. D., Waring, M.
E., Hayes, R. B., Sadasivam, R. S., Mullen, S. & Pagoto, S. (2014).
Evaluating and selecting mobile health apps: strategies for healthcare
providers and healthcare organizations. Translational Behavioral Medicine,
4(4), 363-371. https://doi.org/10.1007/s13142-014-0293-9
Collado-Borrell,
R., Escudero-Vilaplana, V., Villanueva-Bueno, C., Herranz-Alonso, A. &
Sanjurjo-Sáez, M. (2020). Features and Functionalities
of Smartphone Apps Related to COVID-19: Systematic Search in App Stores and Content
Analysis. Journal of Medical Internet Research, 22(8), e20334. https://doi.org/10.2196/20334
Coyne, E., Rands, H.,
Frommolt, V., Kain, V., Plugge, M. & Mitchell, M. (2018). Investigation of
blended learning video resources to teach health students clinical skills: An
integrative review. Nurse Education Today, 63, 101-107. https://doi.org/10.1016/j.nedt.2018.01.021
Domnich, A., Arata, L.,
Amicizia, D., Signori, A., Patrick, B., Stoyanov, S. R., Hides, L., Gasparini,
R. & Panatto, D. (2016). Development and validation of the Italian version
of the Mobile Application Rating Scale and its generalisability to apps targeting
primary prevention. BMC Medical Informatics and Decision Making, 16(83).
https://doi.org/10.1186/s12911-016-0323-2
Duarte-Hueros,
A., Delgado-Morales, C. & Field-Cabezas, N. (2021). Estudio sistemático
sobre distintivos y sellos de calidad de aplicaciones móviles para la formación
en hábitos saludables. En J. Ruiz-Palmero, E. Sánchez-Rivas, E. Colomo-Magaña
& J. Sánchez-Rodríguez (Coords.), Innovación e investigación con
tecnología educativa (pp. 105-116). Octaedro.
Grant, M. J. & Booth, A.
(2009). A typology of reviews: an analysis of 14 review types and associated
methodologies. Health Information and Libraries Journal, 26(2), 91-108. https://doi.org/10.1111/j.1471-1842.2009.00848.x
Hensher, M., Cooper, P., Dona,
W. A., Angeles, M. R., Nguyen, D., Heynsbergh, N., Chatterton, M. L. &
Peeters, A. (2021). Scoping review: Development and assessment of evaluation
frameworks of mobile health apps for recommendations to consumers. Journal
of the American Medical Informatics Association, 28(6), 1318-1329. https://doi.org/10.1093/jamia/ocab041
Jake-Schoffman, D. E., Silfee,
V. J., Waring, M. E., Boudreaux, E. D., Sadasivam, R. S., Mullen, S. P., Carey,
J. L., Hayes, R. B., Ding, E. Y., Bennett, G. G., & Pagoto, S. L. (2017).
Methods for evaluating the content, usability, and efficacy of commercial
mobile health apps. JMIR Mhealth Uhealth, 5(12), e8758. https://doi.org/10.2196/mhealth.8758
Jeminiwa, R. N., Hohmann, N.
S. & Fox, B. I. (2019). Developing a Theoretical Framework for Evaluating
the Quality of mHealth Apps for Adolescent Users: A Systematic Review. The
Journal of Pediatric Pharmacology and Therapeutics, 24(4), 254-269. https://doi.org/10.5863/1551-6776-24.4.254
Lee, C. Y. & Cherner, T.
S. (2015). A Comprehensive Evaluation Rubric for Assessing Instructional Apps. Journal
of Information Technology Education: Research, 14, 21-53. https://doi.org/10.28945/2097
Llorens-Vernet, P. &
Miró, J. (2020). The Mobile App Development and Assessment Guide (MAG):
Delphi-Based Validity Study. JMIR MHealth Uhealth, 8(7), e17760. https://doi.org/10.2196/17760
Martín-Payo,
R., Fernández-Álvarez, M. M., Blanco-Díaz, M., Cuesta-Izquierdo, M., Stoyanov,
S. R. & Llaneza-Suárez, E. (2019). Spanish
adaptation and validation of the Mobile Application Rating Scale questionnaire.
International Journal of Medical Informatics, 129, 95-99. https://doi.org/10.1016/j.ijmedinf.2019.06.005
Messner, E., Terhorst, Y.,
Barke, A., Baumeister, H., Stoyanov, S. R, Hides, L., Kavanagh, D. J., Pryss,
R., Sander, L. & Probst, T. (2020). The German Version of the Mobile App
Rating Scale (MARS-G): Development and Validation Study. JMIR MHealth
Uhealth, 8(3), e14479. https://doi.org/10.2196/14479
Moher, D., Liberati, A.,
Tetzlaff, J., Altman, D. G. & The PRISMA Group. (2009). Preferred Reporting
Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS
Medicine, 6(7), e1000097. https://doi.org/10.1371/journal.pmed.1000097
Nouri, R., Niakan-Kalhori, S.
R., Ghazisaeedi, M., Marchand, G. & Yasini, M. (2018). Criteria for
assessing the quality of mHealth apps: a systematic review. Journal of the
American Medical Informatics Associations, 25(8), 1089-1098. https://doi.org/10.1093/jamia/ocy050
Organización
Mundial de la Salud. (2011). mHealth: new
horizons for health through mobile technologies: second global survey on
eHealth. Global Observatory for eHealth. https://bit.ly/3LV8iVu
Palacios-Gálvez,
M. S., Yot-Domínguez, C. & Merino-Godoy, Á. (2020). Healthy Jeart:
promoción de la salud en la adolescencia a través de dispositivos móviles. Revista
Española de Salud Pública, 94, e202003010. https://doi.org/10.4321/S1135-57272020000100008
Pluye, P., Robert, E., Cargo,
M., Bartlett, G., O’Cathain, A., Griffiths, F., Boardman, F., Gagnon, M. P.
& Rousseau, M. C. (2011). Proposal: A mixed methods appraisal tool for
systematic mixed studies reviews. McGill University. https://bit.ly/3EVOC0f
Powell, A. C., Landman, A. B.
& Bates, D. W. (2014). In Search of a Few Good Apps. JAMA, 311(18),
1851-1852. https://doi.org/10.1001/jama.2014.2564
Saliasi, I., Martinon, P.,
Darlington, E., Smentek, C., Tardivo, D., Bourgeois, D., Dussart, C., Carrouel,
F. & Fraticelli, L. (2021). Promoting Health via mHealth Applications Using
a French Version of the Mobile App Rating Scale: Adaptation and Validation
Study. JMIR MHealth Uhealth, 9(8), e30480. https://doi.org/10.2196/30480
Schulz, K. F. & Grimes, D.
A. (2002). Blinding in randomised trials: hiding who got what. The Lancet,
359(9307), 696-700. https://doi.org/10.1016/S0140-6736(02)07816-9
Stoyanov, S. R., Hides, L.,
Kavanagh, D. J. & Wilson, H. (2016). Development and Validation of the User
Version of the Mobile Application Rating Scale (uMARS). JMIR MHealth
Uhealth, 4(2), e72. https://doi.org/10.2196/mHealth.5849
Stoyanov, S. R., Hides, L.,
Kavanagh, D. J., Zelenko, O., Tjondronegoro, D. & Mani, M. (2015). Mobile
App Rating Scale: A New Tool for Assessing the Quality of Health Mobile Apps. JMIR
MHealth Uhealth, 3(1), e27. https://doi.org/10.2196/mHealth.3422
Terhorst, Y., Philippi, P.,
Sander, L. B., Schultchen, D., Paganini, S., Bardus, M., Santo, K., Knitza, J.,
Machado, G. C., Schoeppe, S., Bauereiß, N., Portenhauser, A., Domhardt, M.,
Walter, B., Krusche, M., Baumeister, H. & Messner, E. M. (2020). Validation
of the Mobile Application Rating Scale (MARS). PLoS ONE, 15(11),
e0241480. https://doi.org/10.1371/journal.pone.0241480
Willis, S., Neil, R., Mellick,
M. C. & Wasley, D. (2019). The Relationship Between Occupational Demands
and Well-Being of Performing Artists: A Systematic Review. Frontiers in
Psychology, 10(393). https://doi.org/10.3389/fpsyg.2019.00393